

GuideLiner-Facilitated Rotational Atherectomy in a Calcified Right Coronary Artery
• Patient Case
A 77-year-old female patient presented with angina on minimal exertion despite receiving optimal antianginal therapy.
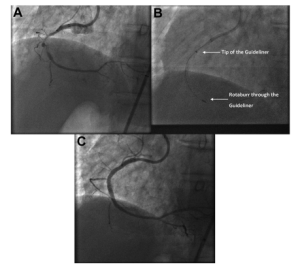
She was referred for percutaneous coronary intervention (PCI) to treat a tight, heavily calcified stenosis in the mid-segment of the right coronary artery (Figure 1A).
A previous PCI attempt had failed because the 1.25-mm rotational atherectomy burr could not cross the calcified lesion (Figure 1B).
• The Procedure
The team used left femoral access, a long sheath, and an Amplatz Left 1 guiding catheter to optimize support.
Initially, the 1.25-mm rotating burr could not cross the stenosis.
A 6-French GuideLiner catheter was then advanced using the “mother-and-child” technique proximal to the stenosis (Figure 1B).
This approach increased the stiffness and support of the guide catheter, wire, and burr assembly, allowing the rotating burr to successfully cross the heavily calcified lesion.
PCI was completed using standard techniques, achieving excellent angiographic results (Figure 1C).
• About GuideLiner
The GuideLiner is a guide catheter extension that enhances support through deep intubation of the target vessel.
It facilitates stent delivery in tortuous or heavily calcified arteries.
Previously, it has been used to retrieve a trapped rotablation burr, but its use to deliver the rotablation burr itself is off-label and reported only once in the literature.
• Safety Considerations
– The rotablation burr should be positioned distal to the GuideLiner before starting forward rotation to prevent damage or shearing of the inner catheter.
– Large burrs should be avoided to reduce the risk of entrapment inside the GuideLiner.
• Conclusion
The GuideLiner can be a valuable adjunct when the rotating burr cannot cross a tight, calcified stenosis.
It provides additional support for the guiding catheter system.
Interventional cardiologists should remain aware of the technical risks and the off-label nature of this application.
